Using a Self-Report Card to Improve Mental Health: Evidence from a clustered Randomized Controlled Trial
Executive Summary
Mental health disorders have become one of the most common and serious chronic diseases in Lebanon where depression followed by anxiety constitute the two biggest mental health burdens. In an attempt to complement the objectives of the 2015-2020 National Mental Health Strategy, Nudge Lebanon in collaboration with The National Mental Health Programme (NMHP) designed and implemented a behavioral intervention to increase the likelihood of mental health patients to follow-up with their health providers. The results suggest that providing patients with a self-assessment card that acts as a reminder to attend their follow-up appointment indeed increases the likelihood that they would attend by around 9 percentage points. Exploratory analysis reveals differences in uptake between new and existing patients, as well as patients with different levels of depression.
Context
Mental Health (MH) disorders are considered one of the top public health concerns around the world. It is estimated that more than 25% of people experience some kind of mental and behavioral disorders during their lifetime [2]. Considering their great impact on the individuals and community’s wellbeing, MH disorders were recognized as a global development priority following the United Nations General Assembly Special Session on Drugs (UNGASS) in 2012.
In Lebanon, latest evidence dating back to 2007 shows the prevalence of severe MH disorders among 4.6% of the Lebanese population, anxiety among 16.7%, mood disorders among 12.6% and suicidal ideation among 4.3%. Overall, around 25.8% of the Lebanese population exhibited some type of mental disorder. Depression was found as the most prevalent MH disorder among the Lebanese with a lifetime prevalence of 9.9%.[1]
In 2015, the Ministry of Public Health (MOPH) Lebanon launched the 2015-2020 National Mental Health Strategy in an effort to integrate Mental Health (MH) into Primary Healthcare (PHC) centers through the National Mental Health Programme (MNHP). One of the main objectives of the MH strategy is to increase the detection, assessment and management of depression which has become one of the most common and serious mental health problems in primary care settings. The strategy provides a cost-effective, evidence-based and multidisciplinary approach to managing depression through a number of steps including diagnosis, patient education and involvement, use of evidence-based medical treatments and an effective collaboration between primary care providers and MH specialists.
Accordingly, social workers and medical staff in 75 PHC centers, were trained by the NMHP to screen patients for depression using the Patient Health Questionnaire (PHQ9). The PHQ9 is a 9-item questionnaire designed to detect the presence and severity of depression. Not only does the PHQ9 help in the early detection of depression, but also in the systematic tracking of a patient’s mental health conditions over time. Therefore, an effective management of depression necessitates consistent follow-up with the healthcare provider to ensure treatment adherence, as well as an assessment of treatment effectiveness.
Against this background, Nudge Lebanon, in collaboration with the NMHP, designed and implemented a behavioral intervention to increase the likelihood of MH patients diagnosed with depression to attend a follow-up assessment with their healthcare provider.
Intervention
The intervention consisted of providing MH patients who were diagnosed with depression (PHQ9 > 4) with a self-report card that tracks their mood changes on a daily basis for a period of two to three weeks, as well remind them of their prescheduled follow-up appointment. The intervention aimed to (a) increase the likelihood of patients to come back for a follow-up assessment, and (b) improve patients’ self-awareness of their daily mood changes and mental health state prior to the appointment date.[2]
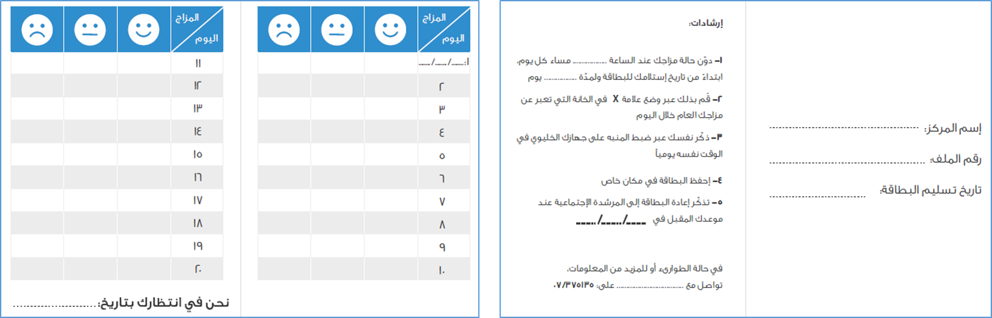
Figure 1: Self-Report Card
The intervention was evaluated using a clustered randomized controlled trial (RCT) with randomization occurring at the visiting day level such that patients screened with depression were randomly assigned into treatment and control days. The final sample consisted of a total of 405 patients who visited the center over 206 days [control days = 105; treatment days = 101]. The distribution of patients into control and treatment is 196 and 209 patients, respectively. Of the 196 patients in control and 209 patients in treatment, 57 and 80 patients in turn came back to the follow-up appointment.
Results
The primary outcome of interest is the likelihood of patients coming back to the follow-up appointment. Additionally, we looked into whether patients show any improvement in their mental health state through the PHQ-9 score, and whether the self-assessment card has improved patient’s self-awareness through daily mood-tracking.
- Follow-up Assessment
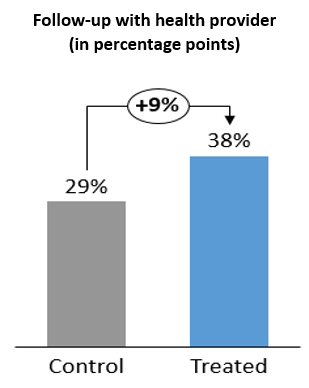
Treated patients were 9 percentage points more likely to attend the follow-up appointment, significant at the 5% level (p-value =0.05). This effect varies between 9 and 5 percentage points with the gradual inclusion of control variables like PHQ9 initial score, age, education, nationality, patient type (exiting or new) and month-of-visit fixed effects.[3] The effect is statistically significant at the 10% level in 5 out of 7 different specifications and represents an increase of 4.7 percentage points with the inclusion of all control variables (p-value=0.31). [4]
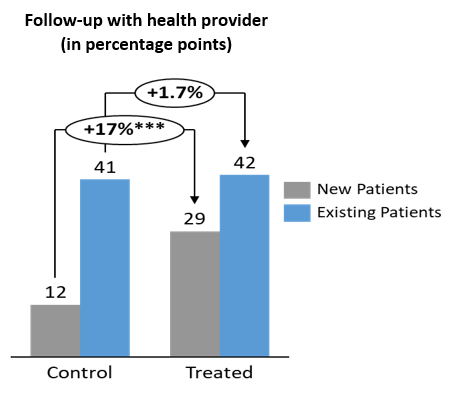 A heterogeneity analysis by patient type suggests that the effect is mostly apparent for new patients (as opposed to existing patients), with a 17 percentage points increase in the likelihood of coming back, significant at the 1% level (p-value =0.009). This effect is robust to the inclusion of control variables (B = 0.147; p-value =0.041).
A heterogeneity analysis by patient type suggests that the effect is mostly apparent for new patients (as opposed to existing patients), with a 17 percentage points increase in the likelihood of coming back, significant at the 1% level (p-value =0.009). This effect is robust to the inclusion of control variables (B = 0.147; p-value =0.041).
In addition to patient type, we also assess differential effects by patient’s depression severity, measured based upon PHQ9 pre score. The analysis reveals a higher impact among patients with mild and moderate depression, as opposed to patients with moderately severe or severe depression. The effect on mild and moderate patients is about 16 percentage points increase in the likelihood of coming back, significant at the 5% and 10% levels respectively (p-value = 0.031, p-value=0.068).[5]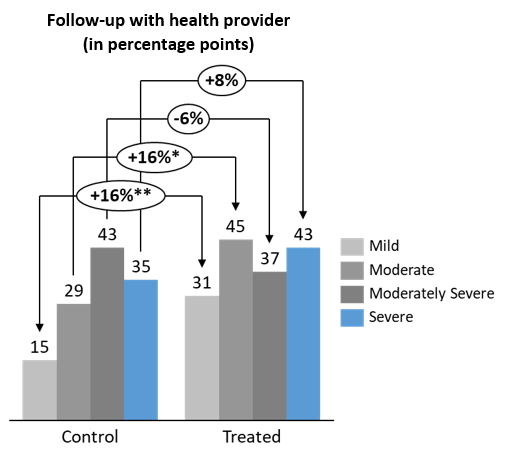
2. Improvement in PHQ9 Score
In addition to the follow-up assessment, we evaluated whether treated patients show a greater improvement in their PHQ9 score compared to control patients. Overall, the analysis which is limited to those who came for the follow-up appointment shows no significant differences between control and treated patients (B = -0.67; p-value =0.59).
3. PHQ9 and Daily Mood Changes
Lastly, we investigate whether there is any association between self-reported mood changes (Happy, Neutral, Sad) and mental health state assessed through PHQ-9 rating score. The analysis is evidently restricted to the treated group who reported their mood changes using the self-assessment card shown in Figure 1. Results reveal a positive relation between the reported number of Sad days and the PHQ9 score. That is, keeping all other factors constant, an additional day reported as Sad is associated with a 1-point increase in the final PHQ9 score.
Conclusion
The findings suggest a great potential for cost-effective interventions to promote the provision of mental health services. Providing patients with a self-assessment card which reminds them of the follow-up appointment and allows them to track their daily mood changes has been found to significantly increase attendance to follow-up appointments. The effect varies between 5 and 9 percentage points and is statistically significant in the majority of specifications.
The assessment yields two more interesting findings. First, a differential effect is observed among new and existing patients whereby treated new patients are significantly more likely to follow up with their mental health provider compared to treated existing patients. Second, it is noteworthy that only Sad versus Neutral mood changes- but not Happy versus Neutral – were shown to significantly explain changes in PHQ-9 scores. We turn to prospect theory’s loss aversion [6] to try to explain this finding. In our context, patients may have a tendency to express feelings of sadness more strongly than to express feelings of happiness, which might help explain the final effect on PHQ-9 captured during the course of the questionnaire.
Given the consequences of mental health disorders on the individual, along with the increase in their lifetime prevalence, there is a pressing need for a collaborative endeavor to strengthen the provision of mental health services and ensure the successful achievement of the strategy objectives.
References
[1] Mental Health and Substance Use, Prevention Promotion and Treatment: Situation analysis and strategy for Lebanon 2015-2020 (2015)
[2] Report: Mental health care in Lebanon: policy, plans and programmes, WHO (2009)
[3] Anxiety and Depression Often Shadow Arab Youth, (2018)
[4] The Burden of Mental Disorders in the Eastern Mediterranean Region, 1990-2013
[5] Fundamental Facts About Mental Health 2015, Mental Health Foundation
[6] Kahneman, D., & Tversky, A. (1979). Prospect Theory: An Analysis of Decision under Risk. Econometrica, 47(2), 263-292.
Endnotes
[1] Lifetime prevalence refers to the percentage of the population who experience the condition at some stage in their lives.
[2] The intervention was conducted at the Amel Association International PHC centre in Bazouriyeh. The center operates under the supervision of the MoPH and was judged to be highly compliant with mental health requirements and procedures.
[3] Although small in magnitude, age is observed to be negatively correlated with the likelihood of attending the follow-up appointment. Also, Lebanese patients are less likely to follow up with their health provider relative to non-Lebanese. As for seasonality effects, patients are more likely to attend follow-up appointments scheduled in the fall season relative to each of winter, spring and summer.
[4] The effect is statistically significant at the 10% level in 4 out 7 specifications after the use of design corrected standard errors due to randomization at the day level.
[5] The effect on mild and moderate patients decreases to 10 and 7 percentage points respectively with the addition of control variables.
You may also like

Increasing Vegetarian Food Consumption at the AUB Cafeteria
